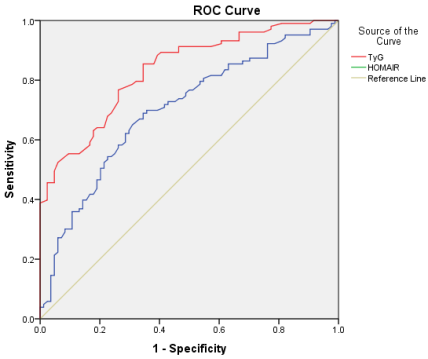
Insulin resistance (IR) is an independent risk factor for type 2 diabetes mellitus (T2DM). Because only triglyceride levels and fasting blood glucose are required to measure the triglyceride-glucose (TyG) index, and the insulin test, which is used in the homeostatic model assessment of insulin resistance (HOMA-IR) calculation, is costly and unavailable in the majority of laboratories in the cities of developing countries. Thus, the goal of our study was compared the predictive power of HOMA-IR and the TyG index for assessing IR, as well as the incidence and prevalence of T2DM. Methods: From January 2025 to July 2025, a cross-sectional study was carried out at Aulaqi Specialized Med. Lab. Several risk factors were evaluated among 215 participants, 110 of whom had T2DM and 105 of whom without diabetes. The following analysis data were collected; high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), triglycerides (TG), fasting blood glucose (FBG), HBA1c, C-peptide, TyG index and HOMA-IR. The results of the statistical test were considered significant if the P value>0.05. Results: The T2DM participants had higher mean TyG index (4.87 ± 0.32 vs. 4.66 ± 0.31, P<0.001) and HOMA-IR (3.07 ± 1.99 vs. 2.32 ± 1.07, P=0.001) values than non-diabetes. In the receiver operating characteristic (ROC) analysis, the TyG index demonstrated a better performance [area under the curve (AUC) 0.832), with 76.7% sensitivity and 73.8% specificity] in predicting T2DM compared to HOMA-IR (AUC 0.700), which had 67.0% sensitivity and 66.7% specificity (P<0.001). Conclusion: The TyG index correlates with HOMA-IR and outperforms it in terms of T2DM detection and prediction, furthermore, the TyG index regarded as useful and valuable surrogate for estimating IR and for predicting T2DM in individuals who appear to be healthy.
| Published in | American Journal of Laboratory Medicine (Volume 11, Issue 1) |
| DOI | 10.11648/j.ajlm.20261101.12 |
| Page(s) | 9-15 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
HOMA-IR, TyG Index, Type 2 Diabetes Mellitus, Insulin Resistance, Diabetes Prediction
Variable | Non T2 DM (n=105) | T2DM (n=110) | P-value |
|---|---|---|---|
n (male/female) | 105 (63/42) | 110 (75/35) | NA |
Age (Years) | 34.42 ± 10.62 | 41.20 ± 12.48 | >0.001* |
Fasting blood glucose (mg/dl) | 90.83 ± 6.88 | 130.34 ± 47.19 | >0.001* |
Total Cholesterol (mg/dl) | 183.35 ± 35.43 | 188.18 ± 39.15 | 0.354 |
Triglyceride (mg/dl) | 148.88 ± 107.82 | 157.68 ± 96.42 | 0. 528 |
HDL-C (mg/dl) | 40.62 ± 8.97 | 42.56 ± 9.20 | 0.133 |
LDL-C (mg/dl) | 115.38 ± 27.41 | 122.36 ± 33.21 | 0.106 |
C-peptide | 3.12 ± 1.32 | 3.46 ± 1.43 | 0.077 |
HbAc1 (%) | 4.79 ± 0.24 | 6.43 ± 1.54 | >0.001* |
HOMA-IR | 2.32 ± 1.07 | 3.07 ± 1.99 | 0.001* |
TyG index | 4.66 ± 0.31 | 4.87 ± 0.32 | >0.001* |
AUC (95% CI) | AUC Std. Error | Sensitivity% | Specificity% | Cut-off | P-value | |
|---|---|---|---|---|---|---|
TyG index | 0.832 (0.776-0. 889) | 0. 029 | 76.7 | 73.8 | 4.70 | >0.001* |
HOMA-IR | 0.700 (0. 625-0.775) | 0. 038 | 67.0 | 66.7 | 2.40 | >0.001* |
TyG Index | HOMA-IR | Total | OR (95% CI) | P-value | |
|---|---|---|---|---|---|
IR | non-IR | ||||
≥ 4.7 | 22 | 21 | 43 | 2.6 (1.138-5.764) | 0.02* |
< 4.7 | 18 | 44 | 62 | ||
Total | 40 | 65 | 105 | ||
TyG | Triglyceride-Glucose Index |
T2DM | Type 2 Diabetes Mellitus |
IR | Insulin Resistance |
HOMA-IR | Homeostatic Model Assessment of Insulin Resistance |
FBG | Fasting Blood Glycose |
TC | Total Cholesterol |
ROC | Receiver Operating Characteristic Analysis |
AUC | Area Under the Curve |
| [1] | Genitsaridi, I., et al., Idf Diabetes Atlas: Global, Regional and National Diabetes Prevalence Estimates for 2024 and Projections for 2050. |
| [2] | Mutie, P. M., et al., An investigation of causal relationships between prediabetes and vascular complications. Nature Communications, 2020. 11(1): p. 4592. |
| [3] | Wen, Z., et al., The role of Triglyceride-Glucose index in predicting pre-DM risk among Chinese adults. Scientific Reports, 2025. 15(1): p. 27101. |
| [4] | Tan, L., J. Liu, and Z. Liu, Association between periodontitis and the prevalence and prognosis of prediabetes: a population-based study. Journal of translational medicine, 2023. 21(1): p. 484. |
| [5] | Lin, J., R. Tu, and Z. e. Lu, Prediabetes and the risk of breast cancer: a meta-analysis. Frontiers in Oncology, 2023. 13: p. 1238845. |
| [6] | Oğuz, İ. S., et al., The Relationship Between the Triglyceride-Glucose Index, and HbA1c and Insulin Resistance in Prediabetic Patients. Age (years). 43: p. 1.05. |
| [7] | Salazar, J., et al., Optimal cutoff for the evaluation of insulin resistance through triglyceride-glucose index: A cross-sectional study in a Venezuelan population. F1000Research, 2018. 6: p. 1337. |
| [8] | Ramalingam, S., A. K. Kar, and R. Senthil, Comparison of triglyceride/glucose index and related parameters with Indian Diabetes Risk Score assessment in non-diabetic individuals visiting primary healthcare centre—A community-based cross-sectional study. Journal of Family Medicine and Primary Care, 2024. 13(1): p. 235-242. |
| [9] | Aman, M., et al., The concordance of triglyceride glucose index (TyG index) and homeostatic model assessment for insulin resistance (Homa-IR) in non-diabetic subjects of adult Indonesian males. Clinical Epidemiology and Global Health, 2021. 9: p. 227-230. |
| [10] | Park, H. M., et al., The triglyceride–glucose index is a more powerful surrogate marker for predicting the prevalence and incidence of type 2 diabetes mellitus than the homeostatic model assessment of insulin resistance. Diabetes research and clinical practice, 2021. 180: p. 109042. |
| [11] | Park, M.-S., Triglyceride-glucose index predicts future metabolic syndrome in an adult population, Korea: a prospective cohort study. Annals of Clinical Nutrition and Metabolism, 2024. 16(3): p. 168-172. |
| [12] | Nahm, F. S., Receiver operating characteristic curve: overview and practical use for clinicians. Korean journal of anesthesiology, 2022. 75(1): p. 25-36. |
| [13] | Samson, S. L. and A. J. Garber, Metabolic syndrome. Endocrinology and Metabolism Clinics, 2014. 43(1): p. 1-23. |
| [14] | Lyssenko, V., et al., Clinical risk factors, DNA variants, and the development of type 2 diabetes. New England Journal of Medicine, 2008. 359(21): p. 2220-2232. |
| [15] | Miller, M., et al., Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation, 2011. 123(20): p. 2292-2333. |
| [16] | Song, K., et al., Prediction of insulin resistance by modified triglyceride glucose indices in youth. Life, 2021. 11(4): p. 286. |
| [17] | Lim JinSook, L. J., et al., Comparison of triglyceride glucose index, and related parameters to predict insulin resistance in Korean adults: an analysis of the 2007-2010 Korean National Health and Nutrition Examination Survey. 2019. |
| [18] | Er, L.-K., et al., Triglyceride glucose-body mass index is a simple and clinically useful surrogate marker for insulin resistance in nondiabetic individuals. PloS one, 2016. 11(3): p. e0149731. |
| [19] | Lee, D. Y., et al., Predictive value of triglyceride glucose index for the risk of incident diabetes: a 4-year retrospective longitudinal study. PloS one, 2016. 11(9): p. e0163465. |
| [20] | Hirschler, V., et al., Ability of TyG index as a marker of insulin resistance in Argentinean school children. Frontiers in Pediatrics, 2022. 10: p. 885242. |
| [21] | Nevárez-Sida, A. and F. Guerrero-Romero, The triglycerides and glucose index: a cost-effectiveness analysis compared with the homeostatic model assessment for insulin resistance. Value in Health Regional Issues, 2023. 37: p. 49-52. |
| [22] | Wan, H., H. Cao, and P. Ning, Superiority of the triglyceride glucose index over the homeostasis model in predicting metabolic syndrome based on NHANES data analysis. Scientific Reports, 2024. 14(1): p. 15499. |
| [23] | Tahapary, D. L., et al., Challenges in the diagnosis of insulin resistance: Focusing on the role of HOMA-IR and Tryglyceride/glucose index. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 2022. 16(8): p. 102581. |
| [24] | Li, M., et al., Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal transduction and targeted therapy, 2022. 7(1): p. 216. |
| [25] | Petersen, M. C. and G. I. Shulman, Mechanisms of insulin action and insulin resistance. Physiological reviews, 2018. |
| [26] | Kurniawan, L. B., Triglyceride-glucose index as a biomarker of insulin resistance, diabetes mellitus, metabolic syndrome, and cardiovascular disease: a review. Ejifcc, 2024. 35(1): p. 44. |
| [27] | DeFronzo, R. A., From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. diabetes, 2009. 58(4): p. 773-795. |
| [28] | Vasques, A. C. J., et al., TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes research and clinical practice, 2011. 93(3): p. e98-e100. |
| [29] | Rong, L., et al., The role of TyG index in predicting the incidence of diabetes in Chinese elderly men: a 20-year retrospective study. Frontiers in Endocrinology, 2023. 14: p. 1191090. |
| [30] | Low, S., et al., The role of triglyceride glucose index in development of Type 2 diabetes mellitus. Diabetes research and clinical practice, 2018. 143: p. 43-49. |
| [31] | Zhang, M., et al., Cumulative increased risk of incident type 2 diabetes mellitus with increasing triglyceride glucose index in normal-weight people: The Rural Chinese Cohort Study. Cardiovascular diabetology, 2017. 16(1): p. 30. |
| [32] | Navarro-González, D., et al., Triglyceride–glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: the Vascular-Metabolic CUN cohort. Preventive medicine, 2016. 86: p. 99-105. |
| [33] | Park, B., H. S. Lee, and Y.-J. Lee, Triglyceride glucose (TyG) index as a predictor of incident type 2 diabetes among nonobese adults: a 12-year longitudinal study of the Korean Genome and Epidemiology Study cohort. Translational Research, 2021. 228: p. 42-51. |
| [34] | Chamroonkiadtikun, P., T. Ananchaisarp, and W. Wanichanon, The triglyceride-glucose index, a predictor of type 2 diabetes development: a retrospective cohort study. Primary care diabetes, 2020. 14(2): p. 161-167. |
| [35] | Lee, J.-W., N.-K. Lim, and H.-Y. Park, The product of fasting plasma glucose and triglycerides improves risk prediction of type 2 diabetes in middle-aged Koreans. BMC endocrine disorders, 2018. 18(1): p. 33. |
| [36] | Li, X., et al., Association between triglyceride-glucose index and risk of incident diabetes: a secondary analysis based on a Chinese cohort study. Lipids in health and disease, 2020. 19(1): p. 236. |
| [37] | Lee SeungHwan, L. S., et al., Predicting the development of diabetes using the product of triglycerides and glucose: the Chungju Metabolic Disease Cohort (CMC) study. 2014. |
| [38] | Du, T., et al., Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovascular diabetology, 2014. 13(1): p. 146. |
| [39] | Guerrero-Romero, F., et al., The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. The Journal of Clinical Endocrinology & Metabolism, 2010. 95(7): p. 3347-3351. |
| [40] | Bastard, J.-P., et al., Evaluation of two new surrogate indices including parameters not using insulin to assess insulin sensitivity/resistance in non-diabetic postmenopausal women: a MONET group study. Diabetes & metabolism, 2012. 38(3): p. 258-263. |
| [41] | Khan, S. H., et al., Metabolic clustering of risk factors: evaluation of Triglyceride-glucose index (TyG index) for evaluation of insulin resistance. Diabetology & metabolic syndrome, 2018. 10(1): p. 74. |
| [42] | Simental-Mendía, L. E., M. Rodríguez-Morán, and F. Guerrero-Romero, The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metabolic syndrome and related disorders, 2008. 6(4): p. 299-304. |
APA Style
Hajar, M. A., Ahmed, S. S., Abdulfattah, B. M. (2026). Triglyceride Glucose Index Is More Robust Surrogate Biomarker for Predicting Type 2 Diabetes Mellitus Than HOMA-IR in Population Attending Aulaqi Specialized Medical Laboratories, Yemen. American Journal of Laboratory Medicine, 11(1), 9-15. https://doi.org/10.11648/j.ajlm.20261101.12
ACS Style
Hajar, M. A.; Ahmed, S. S.; Abdulfattah, B. M. Triglyceride Glucose Index Is More Robust Surrogate Biomarker for Predicting Type 2 Diabetes Mellitus Than HOMA-IR in Population Attending Aulaqi Specialized Medical Laboratories, Yemen. Am. J. Lab. Med. 2026, 11(1), 9-15. doi: 10.11648/j.ajlm.20261101.12
AMA Style
Hajar MA, Ahmed SS, Abdulfattah BM. Triglyceride Glucose Index Is More Robust Surrogate Biomarker for Predicting Type 2 Diabetes Mellitus Than HOMA-IR in Population Attending Aulaqi Specialized Medical Laboratories, Yemen. Am J Lab Med. 2026;11(1):9-15. doi: 10.11648/j.ajlm.20261101.12
@article{10.11648/j.ajlm.20261101.12,
author = {Mohammed Ahmed Hajar and Sami Sultan Ahmed and Basem Mohammed Abdulfattah},
title = {Triglyceride Glucose Index Is More Robust Surrogate Biomarker for Predicting Type 2 Diabetes Mellitus Than HOMA-IR in Population Attending Aulaqi Specialized Medical Laboratories, Yemen},
journal = {American Journal of Laboratory Medicine},
volume = {11},
number = {1},
pages = {9-15},
doi = {10.11648/j.ajlm.20261101.12},
url = {https://doi.org/10.11648/j.ajlm.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20261101.12},
abstract = {Insulin resistance (IR) is an independent risk factor for type 2 diabetes mellitus (T2DM). Because only triglyceride levels and fasting blood glucose are required to measure the triglyceride-glucose (TyG) index, and the insulin test, which is used in the homeostatic model assessment of insulin resistance (HOMA-IR) calculation, is costly and unavailable in the majority of laboratories in the cities of developing countries. Thus, the goal of our study was compared the predictive power of HOMA-IR and the TyG index for assessing IR, as well as the incidence and prevalence of T2DM. Methods: From January 2025 to July 2025, a cross-sectional study was carried out at Aulaqi Specialized Med. Lab. Several risk factors were evaluated among 215 participants, 110 of whom had T2DM and 105 of whom without diabetes. The following analysis data were collected; high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), triglycerides (TG), fasting blood glucose (FBG), HBA1c, C-peptide, TyG index and HOMA-IR. The results of the statistical test were considered significant if the P value>0.05. Results: The T2DM participants had higher mean TyG index (4.87 ± 0.32 vs. 4.66 ± 0.31, P<0.001) and HOMA-IR (3.07 ± 1.99 vs. 2.32 ± 1.07, P=0.001) values than non-diabetes. In the receiver operating characteristic (ROC) analysis, the TyG index demonstrated a better performance [area under the curve (AUC) 0.832), with 76.7% sensitivity and 73.8% specificity] in predicting T2DM compared to HOMA-IR (AUC 0.700), which had 67.0% sensitivity and 66.7% specificity (P<0.001). Conclusion: The TyG index correlates with HOMA-IR and outperforms it in terms of T2DM detection and prediction, furthermore, the TyG index regarded as useful and valuable surrogate for estimating IR and for predicting T2DM in individuals who appear to be healthy.},
year = {2026}
}
TY - JOUR T1 - Triglyceride Glucose Index Is More Robust Surrogate Biomarker for Predicting Type 2 Diabetes Mellitus Than HOMA-IR in Population Attending Aulaqi Specialized Medical Laboratories, Yemen AU - Mohammed Ahmed Hajar AU - Sami Sultan Ahmed AU - Basem Mohammed Abdulfattah Y1 - 2026/01/16 PY - 2026 N1 - https://doi.org/10.11648/j.ajlm.20261101.12 DO - 10.11648/j.ajlm.20261101.12 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 9 EP - 15 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20261101.12 AB - Insulin resistance (IR) is an independent risk factor for type 2 diabetes mellitus (T2DM). Because only triglyceride levels and fasting blood glucose are required to measure the triglyceride-glucose (TyG) index, and the insulin test, which is used in the homeostatic model assessment of insulin resistance (HOMA-IR) calculation, is costly and unavailable in the majority of laboratories in the cities of developing countries. Thus, the goal of our study was compared the predictive power of HOMA-IR and the TyG index for assessing IR, as well as the incidence and prevalence of T2DM. Methods: From January 2025 to July 2025, a cross-sectional study was carried out at Aulaqi Specialized Med. Lab. Several risk factors were evaluated among 215 participants, 110 of whom had T2DM and 105 of whom without diabetes. The following analysis data were collected; high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), triglycerides (TG), fasting blood glucose (FBG), HBA1c, C-peptide, TyG index and HOMA-IR. The results of the statistical test were considered significant if the P value>0.05. Results: The T2DM participants had higher mean TyG index (4.87 ± 0.32 vs. 4.66 ± 0.31, P<0.001) and HOMA-IR (3.07 ± 1.99 vs. 2.32 ± 1.07, P=0.001) values than non-diabetes. In the receiver operating characteristic (ROC) analysis, the TyG index demonstrated a better performance [area under the curve (AUC) 0.832), with 76.7% sensitivity and 73.8% specificity] in predicting T2DM compared to HOMA-IR (AUC 0.700), which had 67.0% sensitivity and 66.7% specificity (P<0.001). Conclusion: The TyG index correlates with HOMA-IR and outperforms it in terms of T2DM detection and prediction, furthermore, the TyG index regarded as useful and valuable surrogate for estimating IR and for predicting T2DM in individuals who appear to be healthy. VL - 11 IS - 1 ER -
Faculty of Medicine and Health Science, Sana’a University, Sana'a, Yemen;Aulaqi Specialized Medical Laboratories, Sana’a, Yemen
Aulaqi Specialized Medical Laboratories, Sana’a, Yemen
Aulaqi Specialized Medical Laboratories, Sana’a, Yemen